Development And Pilot Testing Of A Manual Wheelchair With Independent Positioning Of The Pushrims And Drive Wheels
1-2David Lindenberg, DO, 1-2Andrew Hansen, PhD, 1Eric Nickel, MS, 1-2Gary Goldish, MD
1Minneapolis VA Health Care System, 2University of Minnesotaabstract
A new wheelchair prototype that allowed for independent positioning of the pushrims and drive wheels was developed and pilot tested by three male subjects with spinal cord injuries, who were manual wheelchair users, to determine if changing the horizontal position of the pushrims would alter shoulder biomechanics. Two-dimensional projections of shoulder angles during propulsion with the pushrims set to two different horizontal positions were examined using an 8-camera motion capture system. The results of this study indicate that shoulder extension and shoulder abduction were reduced during the push phase when the pushrims were positioned more anteriorly. These results are pertinent to people with a spinal cord injury or other manual wheelchair users, as these individuals often have shoulder injuries related to wheelchair use. This research may help serve as a guide for future wheelchair design and for clinical optimization of shoulder biomechanics in manual wheelchair users.
background
A reported 1.5 million Americans use manual wheelchairs, according to data from the National Institute on Disability and Rehabilitation Research (Kaye, 2000). Manual wheelchair users rely on their upper extremities for essential daily activities such as wheelchair propulsion, transfers, pressure relief, and household chores. The majority of manual wheelchair users report significant upper limb pain (Curtis, 1999; Gironda, 2004; Ludewig, 2009). The most common pathological process associated with shoulder pain in paraplegic manual wheelchair users is chronic impingement syndrome with subacromial bursitis (Bayley, 1987).
The high prevalence of shoulder injuries in manual wheelchair users is linked to chronic overuse, inefficient propulsion biomechanics, and weight-bearing load during transfers (Gerhart, 1993; Boninger, 2005; Nawoczenski, 2012). Lundqvist et al. (1991) showed that in spinal cord injured patients, severe pain was the only complication that related to lower quality-of-life scores.
Most current manual wheelchairs are propelled by utilization of a pushrim connected directly to the drive wheels, with a common central axle. Although the system is straight-forward and simple, the horizontal adjustability of the axle position is inherently limited, because as the axle is moved forward the chair becomes more vulnerable to tipping backward (Majaes, 1993; Koontz, 2007). Boninger et al. (2000) determined that a more forward position of the drive wheel axle (and pushrims) led to improved wheelchair propulsion biomechanics. Additionally, if the vertical position of the pushrim is too high (or if the seat is too low), the patient has to push with the arms in greater abduction (Koontz, 2007). Van der Woude et al. (1989) found that by adjusting the seat height, an optimal vertical placement of the pushrim for maximum efficiency could be achieved. However, the inherent design of standard wheelchairs has precluded investigation of anterior placements of pushrims that would simultaneously place the drive wheels in positions that compromise the stability of the chair.
PURPOSE
The purpose of this study was two-fold:
- To develop a simple manual wheelchair that allowed for independent positioning of the pushrims and drive wheels; and
- To conduct pilot testing of the new wheelchair prototype by three subjects to evaluate if a more forward position of the pushrims would reduce excess shoulder extension and abduction during the push phase of the propulsion cycle.
While not investigated in this study, the potential clinical benefit of this approach may be a reduction in shoulder pain resulting from manual wheelchair propulsion.
design of the wheelchair
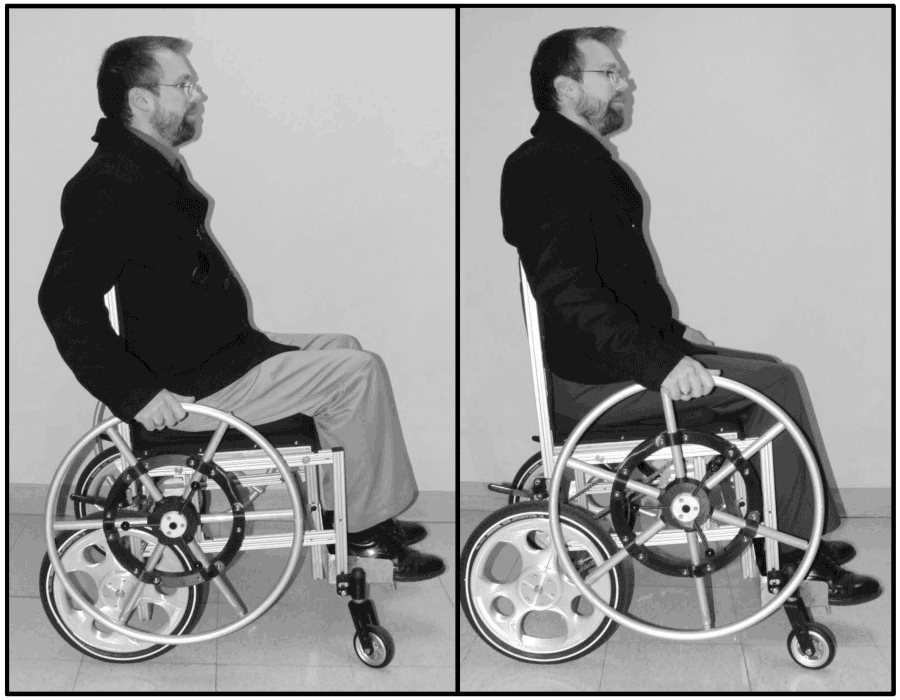 Figure 1. Prototype wheelchair with independently positioned pushrims in (a) posterior/standard and (b) anterior positioning.
Figure 1. Prototype wheelchair with independently positioned pushrims in (a) posterior/standard and (b) anterior positioning.The wheelchair comprises a system with independent control of the fore-aft positioning of the pushrim and drive wheels. Instead of being physically attached, the pushrims and drive wheels are connected by a chain. The position of the pushrims can be adjusted horizontally and/or vertically, as desired for clinical optimization of shoulder biomechanics. The forward position of the pushrims can be positioned in front of the body’s center of mass, without compromising chair stability, as depicted in Figure 1b. The pushrims can easily be disconnected (quick-released) for unobstructed lateral transfers into and out of the wheelchair.
methods
Subjects
The population of interest in this study was veterans with spinal cord injuries occurring at the levels of C7 and below. Three male subjects (S1, S2, and S3) were enrolled. These volunteers met the following inclusion criteria: they could operate a manual wheelchair, they had trunk stability that could be adequately controlled with sub-scapular seat back, and they were between the ages of 18 and 70 years old. Subjects were excluded if they had any of the following: presence of pressure ulcers, upper extremity amputations, or musculoskeletal problems such as shoulder pain that would limit physical ability to perform manual propulsion or multiple transfers. The study was approved by the institutional review board at the Minneapolis VA Health Care System. Subjects provided written informed consent.
Procedures
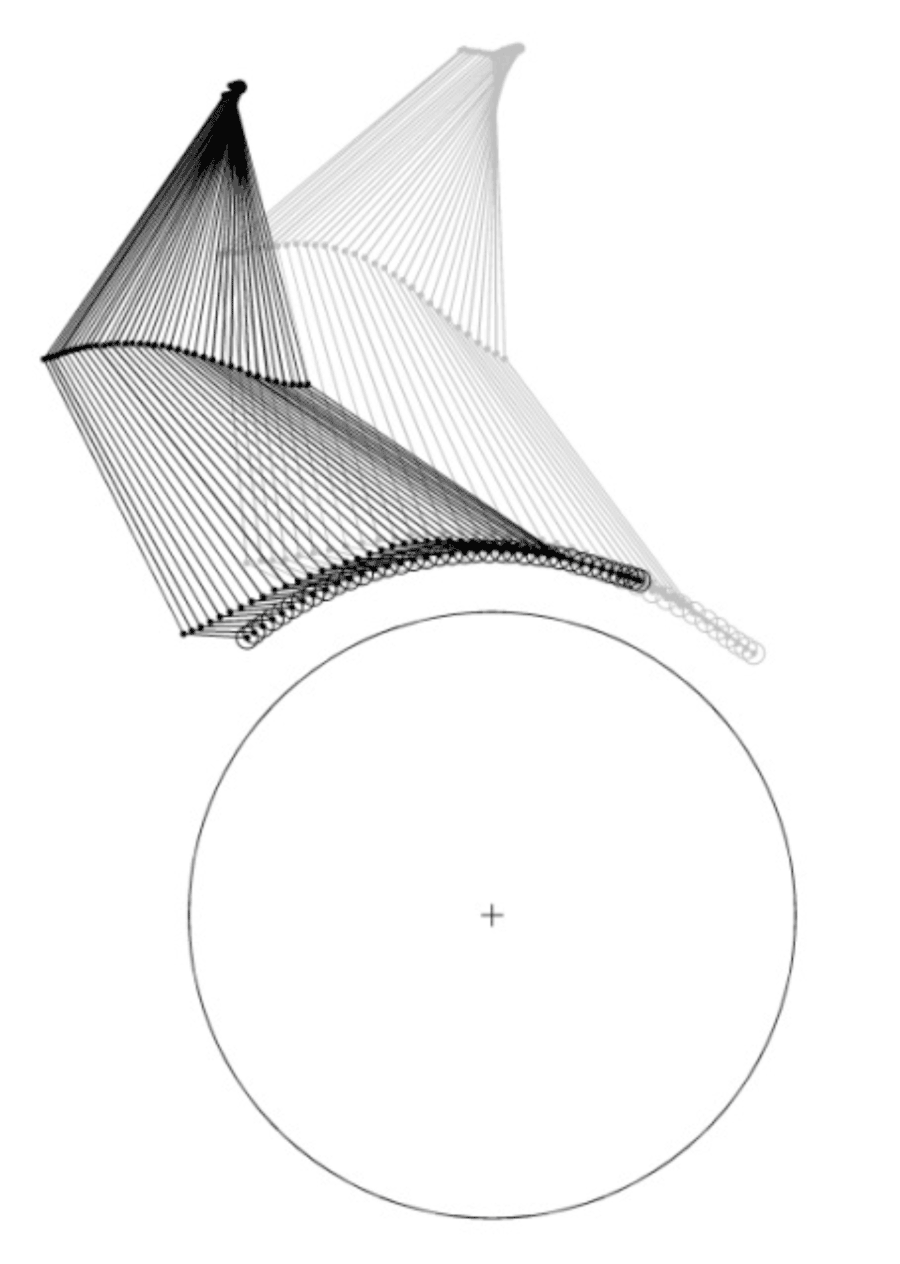 Figure 2. Arm positions of subject S1 during the push phase, for (gray) posterior/standard and (black) anterior pushrim positions.
Figure 2. Arm positions of subject S1 during the push phase, for (gray) posterior/standard and (black) anterior pushrim positions. Physical settings (footrest positions and seat cushion positions) of the wheelchair prototype were adjusted to optimize comfort for each subject. All settings then remained “locked” except for the position of the pushrims. Two positions of the pushrims in the prototype wheelchair were tested, posterior (standard) and a position approximately 18.5 cm anterior to the standard position. The subjects were allowed a short accommodation time for each configuration prior to testing.
Retroreflective markers were placed on the subject’s upper body, including markers on top of the acromio-clavicular joints (shoulders), lateral epicondyles (elbows), medial and lateral sides of the wrists, and on the dorsum of the hands just below the second metacarpals. The marker trajectories were measured using an 8-camera motion capture system (Qualisys, Gothenburg, Sweden). Shoulder angles were approximated as the angles between vertical and two-dimensional projections of lines formed between the shoulder and elbow markers in the sagittal plane (flexion-extension) and coronal plane (abduction-adduction). Data were collected in the center of a 40-foot-long room, as the subject manually propelled the prototype wheelchair with the pushrims in one of the two positions. After a short break, the process was repeated with the pushrims in the other position. The order of pushrim position testing (i.e. posterior and anterior) was randomized.
results
The anterior placement of the pushrims had a dramatic effect on arm movements during the push phase of the propulsion cycle (Figures 2-3). Shoulder extension (Figure 4) and shoulder abduction (Figure 5) at the beginning of the push phase were reduced when pushrims were placed in the anterior position.
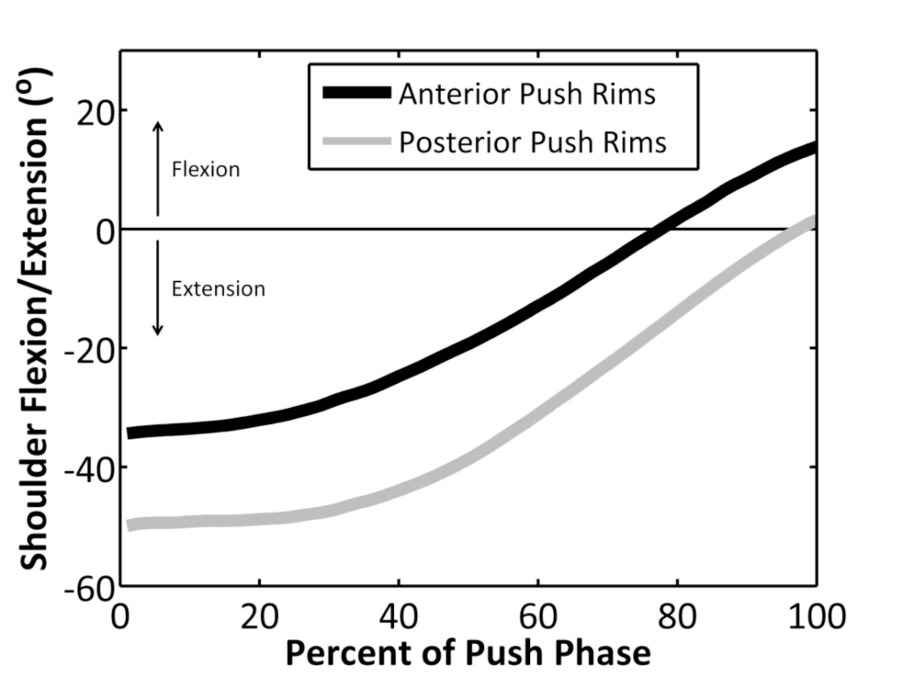 Figure 3. Shoulder flexion and extension angles during the push phase of the propulsion cycle for subject S1.
Figure 3. Shoulder flexion and extension angles during the push phase of the propulsion cycle for subject S1.Subjects provided verbal qualitative feedback on the comfort and ease of use of the new wheelchair. This feedback primarily indicated that the chair felt similar to their standard manual wheelchairs when the pushrims were in the posterior position. It was not difficult for subjects to navigate the chair when the pushrims were in the anterior position. The subjects generally liked the quick-release feature of the pushrim for transfers, and they were able to transfer independently into and out of the chair. The slack in the chain and axle drive did cause some “play” in the pushrim before the wheels turned during initial push. The pushrim spacing in the coronal plane was too wide in the current prototype. Additionally, it was noted that the foot rest was not comfortable.
discussion
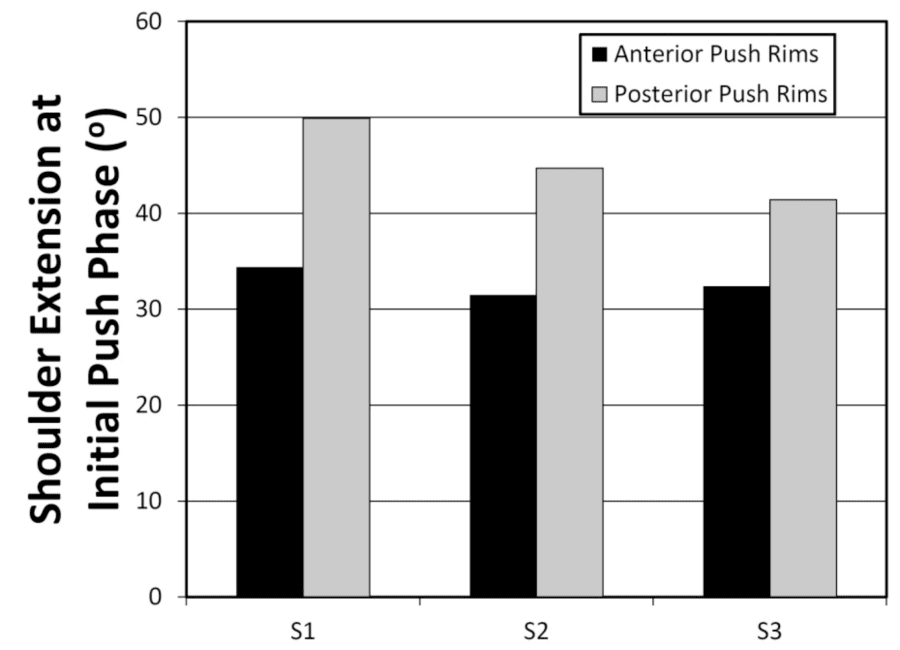 Figure 4. Shoulder extension at initial push phase.
Figure 4. Shoulder extension at initial push phase.The results of this study found that the new wheelchair design dramatically changes shoulder kinematics depending on the horizontal position of the pushrims. The design promotes the use of shoulder angles with reduced shoulder extension and abduction. The clinical significance of these changes should be investigated further in future studies. The expected benefit of optimizing the shoulder angles is to allow for the most efficient and least damaging physiologic positions of the shoulders during propulsion, thereby reducing incidence and severity of shoulder injuries in manual wheelchair users.
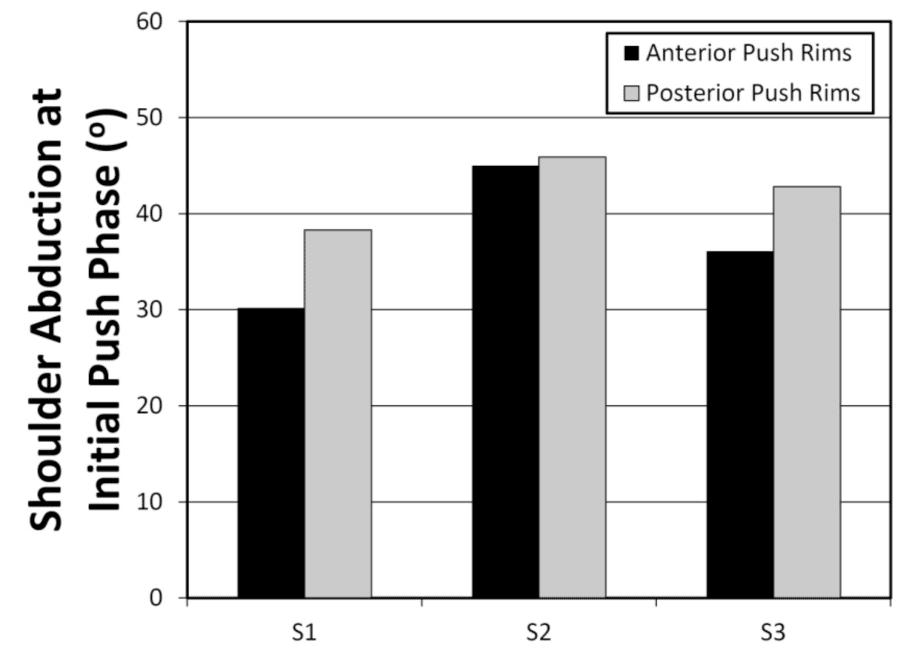 Figure 5. Shoulder abduction at initial push phase
Figure 5. Shoulder abduction at initial push phase Besides reducing shoulder extension and abduction during the push phase, the independent positioning of the drive wheels and pushrims in the new wheelchair design provides a number of other potential advantages over standard manual wheelchair designs. In most standard manual wheelchairs, the large integrated pushrim and wheel combination extends vertically above the level of the seat and obstructs direct lateral access between the wheelchair and transfer surfaces. This obstruction leads to difficulty transferring into and out of the wheelchair because it requires the user to position the wheelchair at an angle with their bed or other transfer surface and then elevate their body a significant distance to clear the wheel of the wheelchair. Manual wheelchair users with spinal cord injuries often lack physical sensation below the waist, making these individuals vulnerable to pressure ulcers and skin breakdown (Byrne, 1996). Trauma and shearing to the buttocks and thighs from the wheel of a wheelchair by failing to clear it during transfers can initiate or exacerbate a wound. The new wheelchair design allows for the removal (quick-release) of the pushrims for easier, unobstructed, lateral transfers into and out of the wheelchair. This feature may further improve shoulder biomechanics during transfers, and it eliminates the possibility of soft tissue contact against the wheel during transfers.
Separating the pushrims from the drive wheels may improve wheelchair users’ hand hygiene because the users’ hands do not inadvertently touch the wheels, which have been in contact with the ground. Future versions of a chain-driven wheelchair system may allow for the incorporation of gears, for down-shifting when going up inclines or across rough surfaces, or when initiating propulsion, and up-shifting for faster propulsion on smooth and level terrain.
Study Limitations
This pilot study involved a small number of subjects. The subjects were allowed only a short accommodation time with the new wheelchair and all of them had years of experience using standard wheelchairs. The wheelchair setup was not optimized for each user because only minimal adjustments were possible with this prototype. Only two positions were studied, posterior and anterior. Two-dimensional projections were examined, as opposed to three-dimensional kinematics; however, our measurements at this stage show that shoulder kinematics are sensitive to pushrim positioning. In this study we did not examine kinetics, efficiency, acceleration, or speed.
Future work is needed with an improved wheelchair design. The qualitative feedback obtained from the subjects in this study will be used to plan the next stage of development of the wheelchair. We anticipate that our next prototype will include upgraded components such as a narrower ultralight wheelchair frame, a better foot rest, slanted seating, and cambered wheels. Studies have utilized three-dimensional tracking systems to study complex shoulder kinematics and to assess impingement risk of various wheelchair-based upper limb exercises (Riek, 2013; Ludewig, 2009). More sophisticated modeling approaches may be useful in future studies to further examine the clinical relevance of a new wheelchair system.
conclusions
The new wheelchair design, which features independent positioning of the pushrims and drive wheels, connected by a chain, has several potential benefits for its users.
- Less shoulder extension and abduction during the push phase can be achieved when the pushrims are positioned anteriorly, as demonstrated in this study. Although the clinical impact of this design has yet to be determined, we hypothesize that (1) an ideal position of the pushrims may exist to allow for optimum shoulder angles during propulsion, (2) the ideal position may entail pushrim positions anterior to the user’s center of gravity, and (3) optimization of the wheelchair-user interface may reduce shoulder injuries.
- Pushrims may be positioned in front of the user’s center of gravity without sacrificing wheelchair stability.
- Quick-release pushrims may allow for easier and safer unobstructed lateral transfers into and out of the chair.
- Hand hygiene may be improved in the new manual wheelchair design because the user’s hands do not contact the wheels during propulsion.
- Gearing may be incorporated into future versions of the wheelchair.
References
Bayley JC, Cochran TP, Sledge CB. The weight-bearing shoulder. The impingement syndrome in paraplegics. J Bone Joint Surg Am. 1987 Jun;69(5):676-8.
Bey MJ, Brock SK, Beierwaltes WN, Zauel R, Kolowich PA, Lock TR. In vivo measurement of subacromial space width during shoulder elevation: technique and preliminary results in patients following unilateral rotator cuff repair. Clin Biomech (Bristol, Avon). 2007;22(7):767–73
Boninger ML, Baldwin M, Cooper RA, Koontz A, Chan L. Manual wheelchair pushrim biomechanics and axle position. Arch Phys Med Rehabil. 2000 May;81(5):608-13.
Boninger ML, Koontz AM, Sisto SA, Dyson-Hudson TA, Chang M, Price R, Cooper RA. Pushrim biomechanics and injury prevention in spinal cord injury: recommendations based on CULP-SCI investigations. J Rehabil Res Dev. 2005 May-Jun;42(3 Suppl 1):9-19.
Byrne DW, Salzberg CA. Major risk factors for pressure ulcers in the spinal cord disabled: a literature review. Spinal Cord 1996; 34:255-63.
Curtis KA, Drysdale GA, Lanza RD, Kolber M, Vitolo RS, West R. Shoulder pain in wheelchair users with tetraplegia and paraplegia. Arch Phys Med Rehabil. 1999 Apr;80(4):453-7.
Gerhart KA, Bergstrom E, Charlifue SW, Menter RR, Whiteneck GG. Long-term spinal cord injury: functional changes over time. Arch Phys Med Rehabil. 1993 Oct;74(10):1030-4.
Gironda RJ, Clark ME, Neugaard B, Nelson A. Upper limb pain in a national sample of veterans with paraplegia. J Spinal Cord Med. 2004;27(2):120-7.
Kaye, H. S., Kang, T., & LaPlante, M. P. Mobility device use in the United States (Disability Statistics Report 14). Washington, DC: National Institute on Disability and Rehabil Research. 2000.
Koontz AM, Spaeth DM, Sichmeler MR, Cooper RA. Prescription of wheelchairs and seating systems. In: Braddom RL. Physical medicine and rehabilitation, 4th ed. Elsevier; 2007. P 373-401
Ludewig PM, Reynolds JF. The association of scapular kinematics and glenohumeral joint pathologies. J Orthop Sports Phys Ther. 2009;39(2):90–104
Ludewig PM, Phadke V, Braman JP, Hassett DR, Cieminski CJ, LaPrade RF. Motion of the shoulder complex during multiplanar humeral elevation. J Bone Joint Surg Am. 2009;91(2):378–89.)
Lundqvist C, Siösteen A, Blomstrand C, Lind B, Sullivan M. Spinal cord injuries. Clinical, functional, and emotional status. Spine (Phila Pa 1976). 1991 Jan;16(1):78-83.
Majaess GG, Kirby RL, Ackroyd-Stolarz SA, Charlebois PB. Influence of seat position on the static and dynamic forward and rear stability of occupied wheelchairs. Arch Phys Med Rehabil. 1993;74:977-82.
Nawoczenski DA, Riek LM, Greco L, Staiti K, Ludewig PM. Effect of shoulder pain on shoulder kinematics during weight-bearing tasks in persons with spinal cord injury. Arch Phys Med Rehabil. 2012 Aug;93(8):1421-30.
Riek LM, Ludewig PM, Nawoczenski DA. How "healthy" is circuit resistance training following paraplegia? Kinematic analysis associated with shoulder mechanical impingement risk. J Rehabil Res Dev. 2013;50(6):861-74
Van der Woude LHV, Veeger DJ, Rozendal RH, Sargeant TJ. Seat height in handrim wheelchair propulsion. J Rehabil Res Dev. 1989;26:31-50.
Acknowledgements
This project was funded by the Mike Utley Foundation and the Department of Veterans Affairs – Rehabilitation Research and Development Service. The authors acknowledge Philip Ebben, Garrett Long, Jacob Polland, Ravinder Diamond, Ruben D’Sa, and Jordan Whitney – for their work on an earlier prototype of this wheelchair. The authors also thank Steve Morin for his assistance in developing the wheelchair prototype and Sara Koehler for her assistance with motion capture.
Audio Version PDF Version